Dr. Paul

Dr. Rebecca

Invisalign®
Finding a dental home by age one is important for your little one’s health. We provide infants ages 0-3 with individualized dental care and instruction in cleaning and oral hygiene. Plus, we have a dedicated infant examination room, and we offer guidance for teething, trauma, prevention, diet, and oh so much more!

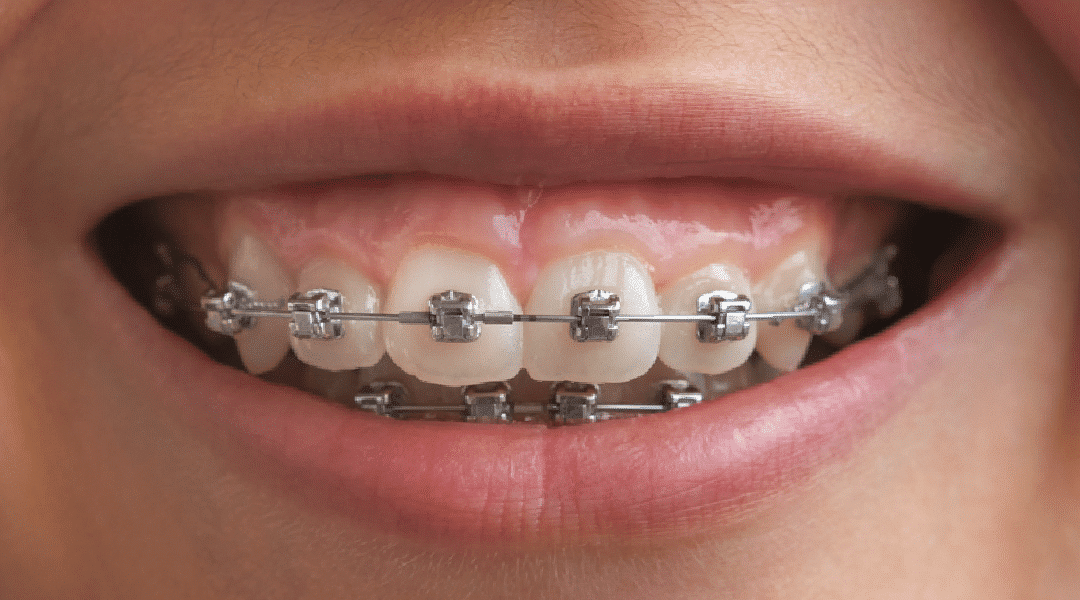
Traditional Braces
Braces are a classic and reliable solution for correcting smiles. Our braces are not only effective but also fashionable, providing a long-lasting way to revitalize your smile.

Clear Braces
Clear ceramic braces use a transparent material with a low-profile design that seamlessly blends with your teeth. They are an ideal choice for individuals looking for a more natural look during their orthodontic treatment.
Self-Ligating Braces
Self-ligating braces feature brackets that open and close like a door, keeping the archwire in place. This technology gently guides your teeth into their optimal positions using ultra-light force. With their discreet design that blends seamlessly with your teeth, you can achieve a beautifully aligned smile in less time!
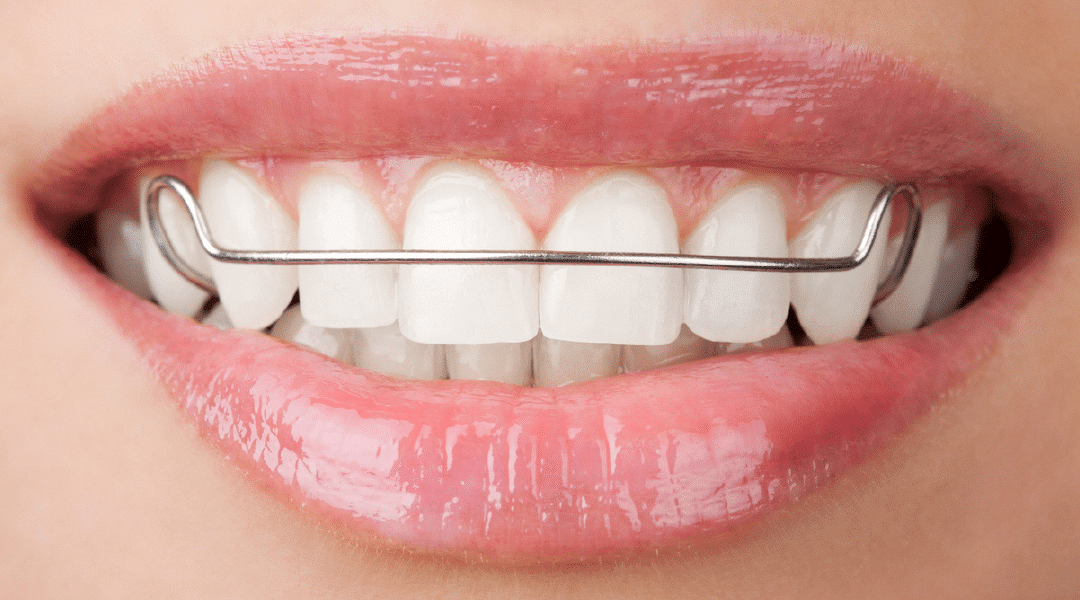
Retainers
After aligning your smile and removing your braces, Lund Orthodontics will provide you with a retainer to preserve your stunning new smile for years to come. Whether you opt for a permanent or removable retainer, our team will work with you to select the best type based on your individual needs.